Fronto-temporal Dementia (FTD)
FRONTO-TEMPORAL LOBE DEMENTIA BASICS
WHAT IS FRONTO-TEMPORAL DEMENTIA?
FTD (also known as Pick’s Disease) is a term used to describe a form of dementia that causes neuronal death and progressive damage to the frontal and temporal lobes of the brain. It is characterized by behavioral and personality changes along with a decline in the ability to empathize, learn, reason, make judgments, communicate, and eventually carry out daily activities.
The frontal lobes of the human brain, which is located directly behind our forehead is responsible for controlling behavior, emotion, attention, judgment, planning, and self-control. Damage to this area leads to reduced intellectual abilities and changes in personality, emotion, and behavior. The temporal lobes of the human brain on the other hand are responsible for processing language, especially what we hear and see. Damage to these areas primarily leads to difficulty understanding or expressing language.
FRONTO-TEMPORAL VS. ALZHEIMER'S

Although comparatively less prevalent than Alzheimer’s, Parkinson’s, or other neurodegerative diseases, which usually affects individuals who are of a more advanced age, for FTD, age is just a number. It can strike when people are as young as in their mid 20s and is usually diagnosed between 45 and 65 years old. As such, FTD may end up having a larger impact on the patients life and those around them over the course of the illness.
The first signs of FTD tend to manifest themselves with impairments to their behavior and emotions such as depression, poor judgement, lack of inhibition, repetitive compulsive behavior. In contrast, Alzheimer's early symptoms are primary memory loss.
To compare types of dementia's - visit our Compare Diagnosis Page or visit these diagnosis specific pages:
FRONTO-TEMPORAL VS. OTHER TYPES OF DEMENTIA
Obtaining a clear diagnosis for dementia is extremely difficult for physicians.
Misdiagnosis and undiagnosed is common in dementia because while brain imaging, blood testing, and comprehensive tests can help in the diagnosis, it is still not a perfect science. Physicians rely on the tests as well as the progressing deterioration and occurrence of different symptoms to make as best of a diagnosis and treatment plan as possible.
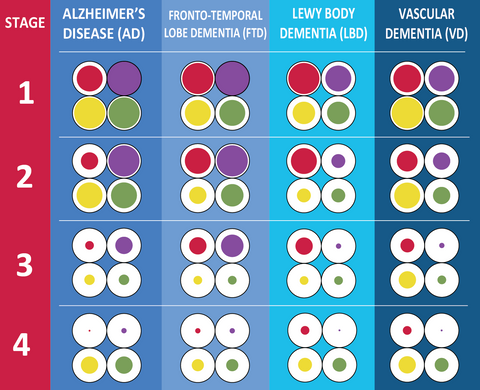
While there are many types of dementia, the four largest subset of dementias are Alzheimer's (estimated at 60%-80% of the cases), Fronto-temporal Lobe Dementia (estimated at 5-10% of cases), Lewy Body Dementia (estimated at 5-10% of cases), and Vascular Dementia (estimated at 10-20% of cases). Mixed dementia - or having multiple types of dementia (example: Alzheimers and Fronto-temporal Lobe) is also common in dementia patients, making it even more complex to diagnose and treat.
Although it varies from patient to patient, FTD specifically compared to other symptoms shows itself primarily with behavior changes in the initial stages. Depression, apathy, subtle mood changes, inappropriate behaviors, and minor memory loss are all signs of the early stages of FTD. When compared to Alzheimer's or some of the other types of dementia, the behavioral changes are more prevalent then the memory loss manifested in Alzheimer's, drastic mood changes in a short amount of time and hallucinations in Lewy Body Dementia, to the more aggressive physical impairments or motor loss if they have Vascular Dementia.
Towards the middle and later stages, advanced behavioral issues such as aggression, anxiety, wandering and progressed memory loss is typical of an FTD patient. Impaired speech and difficulties with language such as word finding and word association is also common, similar to Alzheimer's, although behavioral issues tend to be more pronounced. Depending on the form of FTD and if there is a mixture of dementias, the patient may experience motor difficulties very early on, or towards the later stages.
Being informed about the other types of dementias and symptoms experienced by those who have it, assists in the diagnosing and treating of the disease. It is extremely important to take note of the progressive changes of symptoms as this will enable the physician to make customized treatment and medication plans to counter the symptoms of the disease.
This chart compares the symptoms of the different types of diseases to show what types of symptoms are more or less in the various diseases.

For more information on comparing the different types of dementia's - visit our Compare Diagnosis Page or visit these diagnosis specific pages:
SYMPTOMS & STAGES OF FRONTO-TEMPORAL DEMENTIA
The progress of FTD can vary dramatically from person to person. There are both cases of accelerated progression of just a couple of years as well as rates of much slower progression where a patient deteriorates over more than a decade. But on average the symptoms progress and become more pronounced over a course of 8 to 10 years.

The symptoms of FTD depend on the area of the brain that is affected. In contrast to Alzheimer’s, memory often remains unaffected until the later stages. And although during the initial stages, a person may exhibit distinct symptoms based on the area of brain that is first damaged, over time, as the dementia progresses, the symptoms converge. If the frontal lobes are affected first, changes in behavior and personality become apparent. This is called Behavioral-Variant FTD.
On the other hand, if the temporal lobes are affected first, the loss of language skills becomes obvious. This is known as Primary Progressive Aphasia. Within it, there are two types: progressive non-fluent aphasia and semantic dementia. In progressive non-fluent aphasia, the person’s speech becomes hesitant and lacks grammatical accuracy. In semantic dementia, patients lose their ability to understand or formulate words in a spoken sentence.
Stage 1: Cognitive Impairment
Stage 2: Early Stages
Behavioral-Variant FTD
Progressive Non-Fluent Aphasia
Semantic Dementia
Stage 3: Middle Stages
Behavioral-Variant FTD
Progressive Non-Fluent Aphasia
Semantic Dementia
Stage 4: Late Stages
Behavioral-Variant FTD
Progressive Non-Fluent Aphasia
Semantic Dementia
After four to five years from onset, symptoms are usually quite advanced. This means that the patient’s language skills would be barely existent, making communication extremely difficult.
It's important to note that those diagnosed with Fronto-temporal Dementia can show symptoms from each of these types or they may have FTD mixed with another type of dementia as well.

CAUSES, DIAGNOSIS, TREATMENTS
For more detailed information about Fronto-temporal Lobe Dementia including it's causes, how to detect and diagnose the disease, treatments, care options, and important resources for families caring for a loved one, check out our Guide at this link!
CAREGIVER TOOLS
FRONTO-TEMPORAL CARE TIPS
Care Tips on dealing with every aspect of Fronto-temporal Dementia (FTD) care including how to keep your loved one safe, how to choose the right care home or tips on how to keep them at home and independent as long as possible.
Causes of FTDDetection & Diagnosis of FTDPrevention of FTDResearch of FTDSymptoms of FTDTreatments for FTD
ASSISTIVE PRODUCTS FOR FRONTO-TEMPORAL DEMENTIA
Find assistive products for Fronto-temporal Dementia in our Fronto-Temporal Dementia Products page. Sort by stage and symptoms to find the best products for you or your loved one.
Products by Stage:
|
Products by Symptom:
|
CARE ARRANGEMENTS

In terms of care arrangements for FTD patients, there are generally two types of options that the patient’s friends and family can opt for: in-home care or out-home care.
During the initial stages, while the patient is still able to function independently, most people may prefer to remain at home, where they are most familiar with their surroundings.
After initial diagnosis, the primary caregiver may still be able to handle the tasks of looking after the patient. But as the symptoms progress to the early and middle stages, they can opt for in-home care arrangements. There are several types available in this category:
- Companion services – to help with supervision and recreational activities.
- Personal carers – to help with various personal care tasks such as bathing, dressing, eating, and exercising.
- Homemaker services – to help with housekeeping, cooking, or shopping.
- Medical carers – to help with medical needs, physical, and/or mental therapies
Another option for patients who are still able to function relatively independently, is Adult Day Care Centers. These facilities provide a safe environment for dementia patients to pursue activities, interests, and socially interact with people. This type of care arrangement can give the patients a sense of freedom while dealing with their diagnosis. They are also likely to have counselling, health services, meal services, personal care, behavior management, therapy, and other related services available.
During the last stages of dementia, when the patient is unable to fend for themselves, the best choice often will be residential care in the form of Personal Care Homes, Assisted Living, Nursing Homes with special care or memory units. There, they can receive specialized care and treatment to ease their situation. Each of these facilities will offer different levels of care. Selecting one will depend on the patient’s needs and progression of FTD. Read our detailed guides on each one to assess which may be the best fit for you or your loved one.
Hospice Care and Geriatric Psychiatric Facilities are two lesser talked about short-term arrangements for patients with dementia. These systems assist with end of life comfort measures (hospice) and medication rebalancing (Geriatric Psychiatric Unit), both of which are crucial to maintaining the patient’s dignity and safety for them and their caregivers.
Hospice Care services are available with any care arrangement and are attached to the patient wherever they go as long as the organization providing the services is able to provide services.
Geriatric Psychiatric Facilities are meant to be a resource for when a patient is experiencing severe behavioral changes that need to be adjusted for with medication in order to ensure the patients, and his/her caregivers safety.
For more information on the differences, how to find a care facility and on commonly experienced issues with each care arrangement, visit the following pages:
- Care at Home
- Adult Day Care
- Assisted Living
- Nursing Home
SUPPORT & RESOURCES
You are NOT alone. Rest assured, there are many out there who have been in your shoes and who want to help you through this tough time. Here are a couple of resources available to connect with others who are going through what you are going through:
- Association for Frontotemporal Degeneration: Support Group Listing
- Online Forums & Chat Rooms:
- University of California, Aging and Memory Center: FTD Support Forum
- Alzheimer's Association Forum: AlzConnected
- Facebook Groups:
- Dementia Information
- Frontotemporal Dementias Info and Support
- Forget Me Not - Frontotemporal Dementia (FTD)
- The Association for Frontotemporal Degeneration (AFTD)
- Hidden Group for Young Adults: Association for Frontotemporal Degeneration (AFTD) - Young adult Facebook group for people in their 20s and 30s who have a family member or loved one with FTD. This group serves as a supportive online forum and gathering place for young adults. To join the “secret” group, please email youngadults@theaftd.org and include the email address you used to open your Facebook account. You can expect an invite to join the group within a week.
- FTD Spouse Caregiver Support Yahoo Group An independent, online, peer support group committed exclusively to the spouses of those diagnosed with frontotemporal degeneration and early-onset dementias.
- Anonymous chat rooms for Free therapy: 7 Cups
- Informal Caregiver Connections: Sometimes AFTD can match FTD caregivers in a particular city or region through information they share when they register. It is an informal connection that can be helpful if there are no face-to-face groups available. AFTD identifies people in the network who are in a similar situation and within a reasonable distance from you. After agreement by both parties, AFTD shares a name and a contact number or email, but no other personal information. You take it from there. To request a search, please contact AFTD’s HelpLine at info@theaftd.org or toll-free 866-507-7222. You can also register with AFTD on-line.
FRONTO-TEMPORAL DEMENTIA ORGANIZATIONS
For family members and friends who would like to educate themselves further on the details of FTD, its symptoms, treatments, and challenges, you should seek the assistance of local or national dementia association. Below are some resources to help start your research:
Radnor Station Building #2 Suite 320
290 King of Prussia Road
Radnor, PA 19087
info@theaftd.org
http://www.theaftd.org
1-800-272-3900 (toll-free)
1-866-403-3073 (TTY/toll-free)
info@alz.org
www.alz.org
National Institute on Aging (NIA)
National Institutes of Health, DHHS
31 Center Drive, Rm. 5C27 MSC 2292
Bethesda, MD 20892-2292
http://www.nia.nih.gov
FRONTO-TEMPORAL DEMENTIA RESEARCH
FINDING A PHYSICIAN
For a list of providers or resources close to your area that specialized in FTD, follow this link.
Also, although these are centers that for the most part specialize in Alzheimer's - they can serve as a starting point for more information and resources. Follow this link to search for centers in your area.
CLINICAL TRIALS
FTD is still a rather poorly understood illness and often leads to under- or mis-diagnosis. One of the best ways to better understand FTD is to study the disease more in-depth. And to do that, participating in research and clinical trials can be very beneficial. In addition to helping to advance the understanding of FTD, patients can often benefit from the clinical trials. Below are a few types of studies that can be found:
- Treatment trials – where new and existing drugs are tested to study its effects on FTD symptoms
- Genetics studies – where scientists look into a possible genetic connection to the illness
- Diagnostic studies – where researchers seek better and improved methods of diagnosing FTD
- Prevention trials – where researchers investigate for ways to prevent the onset of FTD itself
FINDING CURRENTLY RECRUITING CLINICAL TRIALS AND STUDIES
- AFTD maintains a listing of Currently Recruiting Clinical Trials and Studies, updated quarterly.
- ClinicalTrials.gov – maintained by the U.S. National Institutes of Health (NIH) of federally and privately funded clinical research, the registry provides patients, family members, and members of the public easy and free access to information on clinical studies for a wide range of diseases and conditions. A search feature lets you look specifically for studies in FTD. Enter “frontotemporal degeneration”, “frontotemporal dementia”, or search terms for the specific FTD disorders: primary progressive aphasia, progressive supranuclear palsy, cortical basal degeneration, or ALS and FTD to view a full list of all registered trials, eligibility criteria, participating medical centers and contact information for each.
- NIH Clinical Center – conducts research in a wide range of diseases, including frontotemporal dementia. The Clinical Center’s website is designed to help people learn more about clinical trials, why they matter and how to participate. In addition, health care professionals can read about evidence-based strategies for talking with patients about trials, and find audience-tested posters to help promote trials in clinics and offices.
- ARTFL Network – a consortium of academic medical centers partnered with patient support organizations conducts clinical research in sporadic and familial FTD. ARTFL is funded by the National Institutes of Health and is part of the Rare Diseases Clinical Research Network.
- LEFFTDS – conducts longitudinal studies of people in families who have inherited a pathogenic mutation in progranulin, C9ORF72, or tau. A primary goal of LEFFTDS is to identify the most robust and reliable methods to track disease progression in familial FTD so that disease-modifying therapeutic trials can be designed appropriately.
You might be interested in...
View all-

Making Public Outings Easier With Dementia Comm...
Making Public Outings Easier With Dementia Communication Cards Imagine you're out in public. Your loved one with dementia is confused, anxious, or repeatedly asking questions. They may have difficulty understanding...
Making Public Outings Easier With Dementia Comm...
Making Public Outings Easier With Dementia Communication Cards Imagine you're out in public. Your loved one with dementia is confused, anxious, or repeatedly asking questions. They may have difficulty understanding...
Read more -

Traveling With Dementia: 12 Things We Learned t...
Traveling with dementia can feel overwhelming, but a little preparation can make the journey safer, calmer, and more manageable for everyone involved. The first time we traveled with my dad...
Traveling With Dementia: 12 Things We Learned t...
Traveling with dementia can feel overwhelming, but a little preparation can make the journey safer, calmer, and more manageable for everyone involved. The first time we traveled with my dad...
Read more -

When Depression Isn't Just Depression: Early Si...
When Depression Isn't Just Depression: How Depression Can Sometimes Hide Dementia Depression, apathy, and dementia can look surprisingly similar. Understanding the difference can help families know when to ask deeper...
When Depression Isn't Just Depression: Early Si...
When Depression Isn't Just Depression: How Depression Can Sometimes Hide Dementia Depression, apathy, and dementia can look surprisingly similar. Understanding the difference can help families know when to ask deeper...
Read more



Disclaimer
All text, charts, graphics, images, videos, downloads, and tools on this page (“Content”) are for general educational purposes only and are not medical advice. Dementia varies by person and diagnosis is complex; summaries and comparisons are simplified. We do not guarantee accuracy or completeness. Use at your own risk. To the fullest extent permitted by law, Dementia Aide LLC disclaims liability for any loss or damages arising from use of or reliance on the Content.
Copyright: © 2026 Dementia Aide LLC. All rights reserved.